
Clinical trials bring good news on non-surgical valve replacement
Transcatheter aortic valve implantation (TAVI) has been in use for more than 20 years. So what have we learned about its outcomes, compared to open-heart valve replacement surgery? This review of three clinical trials shows excellent results and allays concerns that the prosthetic valves used in TAVI could be less durable than those used in surgery.
Heart valve disease is one of the most frequent cardiovascular diseases and it affects more than one million people (3.5% of the population) in Canada. The incidence of heart valve disease is expected to grow exponentially in the next decade due to the aging of the population. Aortic valve stenosis, which is a narrowing of the aortic valve, one of the four heart valves, is the most frequent heart valve disease and is directly responsible for 3,000 deaths and 10,000 procedures in Canada every year. No medication has yet been proven to slow or halt the progression of heart valve disease so the only option to treat severe aortic valve stenosis is to replace the failing aortic valve with a prosthetic heart valve, the most common being a bioprosthetic valve which is made using either cow or pig heart tissue.
For many decades, the standard treatment of aortic valve stenosis has been to perform open-heart surgery to replace the aortic valve by a prosthetic valve. However, about 20 years ago, a new revolutionary treatment was introduced, which is the implantation of a prosthetic valve through a catheter, without surgery. This is called transcatheter aortic valve replacement (TAVR) or implantation (TAVI). TAVI is a valuable and less invasive alternative to surgery. Several randomized clinical trials have been conducted in the past two decades to validate this new technology for clinical use.
Trials tested different elements
These clinical trials were first performed in patients with high or extreme surgical risk, and then in patients with intermediate surgical risk, and more recently in patients with low surgical risk, who represent about 65% of the population that required aortic valve replacement. There are two main types of prosthetic valves that can be used for TAVI: balloon expandable valves and self-expanding valves. The trials conducted in patients with low surgical risk include:
• PARTNER 3, which compares TAVI with a balloon-expandable valve versus surgery
• EVOLUT-LR, which compares TAVI with a self-expanding valve versus surgery
• NOTION, which compares the first generation of self-expanding TAVI versus surgery.
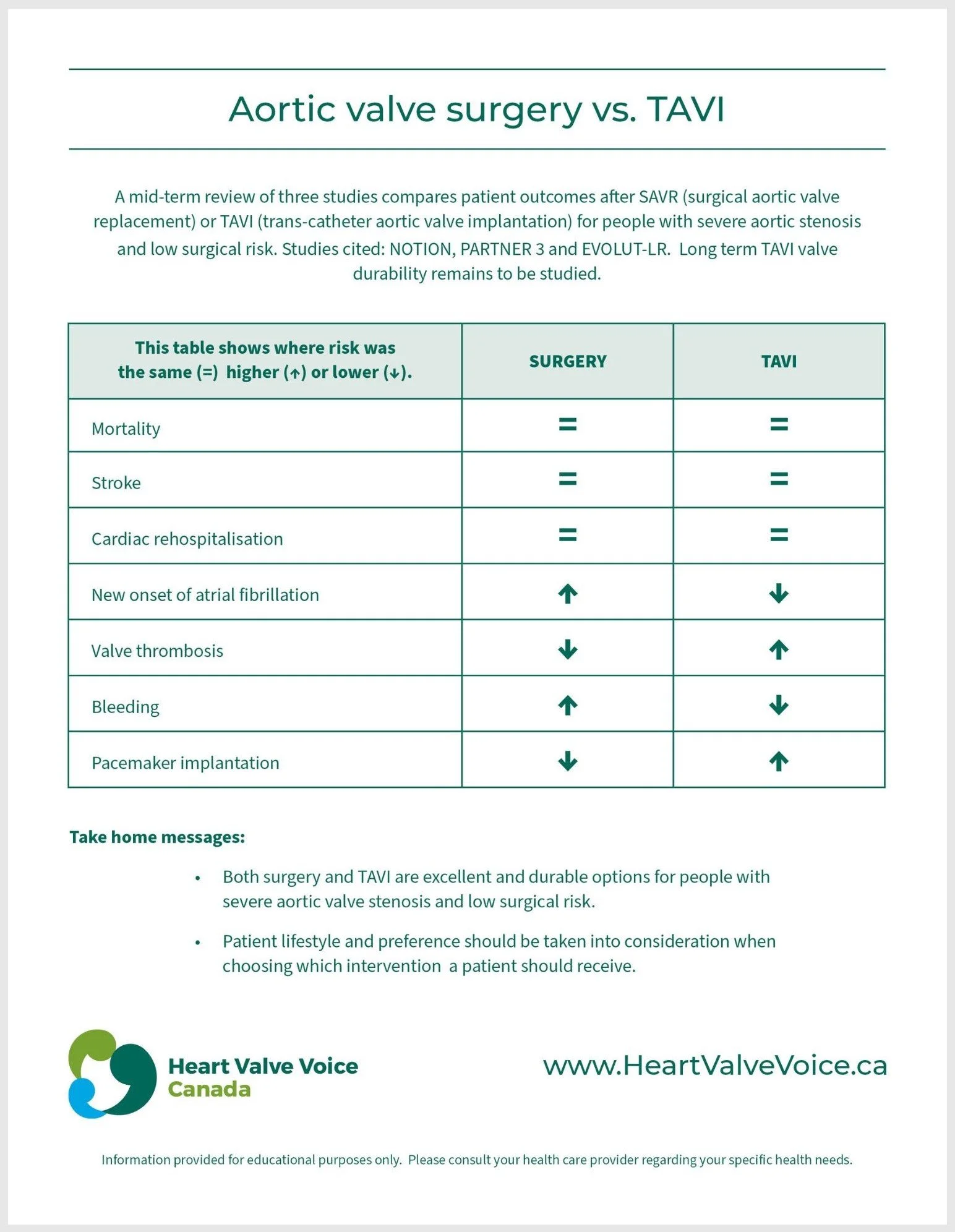
The primary results of these three trials have been previously reported, and the primary outcome was the rates of mortality, stroke and cardiac rehospitalization at one or two years following intervention. The purpose of this report is to describe the results of these trials at five years follow-up for PARTNER-3, four years for EVOLUT-LR, and ten years for NOTION.
Follow-up results positive
Overall, the survival rates in these trials were excellent, similar in both types of aortic valve replacement, and similar to those in the general population of the same age and without heart disease. The rate of stroke was also low and similar in both groups. The rate of rehospitalization because of cardiac complication was lower in TAVI versus surgery during the first year of follow-up, but thereafter it became similar in both groups.
In the PARTNER 3 trial, the percentage of patients alive and well, which refers to patients who are alive at five years with a good quality of life, was high and similar in both groups: 71% with TAVI versus 72% in surgery. The rate of failure of the prosthetic valve was low and similar in both groups at five years: 3.3% with TAVI versus 3.8% with surgery.
All three trials demonstrated an excellent and similar durability of TAVI versus surgery prosthetic valves. However, the follow-up duration of PARTNER 3 and EVOLUT LR was limited to five years, which is not sufficient to draw definitive conclusions regarding the long-term durability of TAVI prosthetic valves.
The NOTION trial, on the other hand, had a 10-year follow-up and reported similar and excellent valve durability in TAVI versus surgery. However, the patients in the NOTION trial were older and had therefore shorter life expectancy; only 35% of these patients were still alive at ten years. Furthermore, it's important to emphasize that the prosthetic valves employed in this trial are no longer in use. Therefore, the results of the NOTION trial need to be confirmed by other trials.
Complications vary
With regard to the other complications, some were more frequent in TAVI and others more frequent in surgery. In particular, valve thrombosis (clotting on the valve), was more frequent with TAVI but was generally reversible with treatment and was without consequence for the patient. The incidence rate of atrial fibrillation, a cardiac arrhythmia characterized by irregular and rapid heartbeats, was higher in patients who underwent surgery. Serious bleeding was more frequent with surgery. In the EVOLUT-LR trial, which used a self-expanding valve, the rate of pacemaker implantation was more frequent with TAVI versus surgery.
Excellent results overall
In summary, the news is good and these three clinical trials revealed that at mid-term follow-up, TAVI compares favorably with surgical valve replacement, with excellent results with both types of treatment in terms of survival, durability of the valve and other complications.
In the early days of TAVI, some concerns were expressed that this type of prosthetic valve would be less durable than the valves used for surgical valve replacement. These initial concerns are not confirmed by the results of the mid-term follow-up of these recent trials. The valve durability appears to be excellent and similar or even somewhat better compared to surgery at five-year follow-up. This is, however, not a definitive conclusion and longer-term follow-up is needed to confirm that the durability of TAVI matches or exceeds that of surgery.
It should be noted that women accounted for only one-third of the patients included in the PARTNER 3 and EVOLUT-LR clinical trials, and further clinical trials are thus necessary to confirm these results in women. In this regard, the primary results of the RHEIA clinical trial, comparing TAVI and surgery in women with severe aortic stenosis, will be presented in 2024.
Implications for people living with aortic valve stenosis
First, it is important to determine the optimal timing of the aortic valve replacement procedure for the individual patient, this is done collaboratively with the patient during a follow-up visit every year or every six months, ideally performed in a dedicated clinic by a team of specialists in heart valve disease. In the patients referred to a heart valve center for an aortic valve intervention, the next step is to decide which is the best type of valve replacement, i.e. surgery or TAVI, and the best type of valve for the patient. This process should be a shared decision between the treating physicians and health care professionals, the Heart Team (a team of specialists including cardiologists, cardiac surgeons and other disciplines), and also, importantly, the patient and their family and caregivers.
Several factors should be taken into consideration for selecting a surgery or TAVI, including:
· the age of the patient
· the level of surgical risk
· the expected life expectancy and lifestyle of the patient.
In people older than 80 years old and/or with high surgical risk, TAVI is generally preferred over surgery. In people younger than 65 and with low surgical risk, surgery is generally recommended. In those aged between 65 and 80 and/or with intermediate surgical risk, the decision between surgery versus TAVI should take into account other factors and, in particular, patient’s preferences.
In conclusion, both surgery and TAVI are excellent and durable options for people with severe aortic valve stenosis and low surgical risk. The patient should have an important voice and weight in the decision between surgery versus TAVI and should feel comfortable asking questions and expressing their preferences depending on their lifestyle and aspirations following aortic valve replacement.
Take home messages
· Both surgery and TAVI are excellent and durable options for people with severe aortic valve stenosis and low surgical risk.
· Patient lifestyle and preference should be taken into consideration when choosing which intervention a patient should receive (surgery vs TAVI).
This report was prepared for Heart Valve Voice Canada by John Stott (Patient), Sébastien Hecht (PhD Candidate*), Marie-Ange Fleury (PhD Candidate*), Nancy Côté (PhD, Adjunct Researcher*), and Philippe Pibarot (D.M.V., Ph. D., FAHA, FACC, FESC, FASE, FCCS, Professor at the Department of Medicine, and Head of Cardiology Research*).
*Quebec Heart and Lung Institute, Quebec City, Province of Quebec, Canada.